

Drugs Part 1

I just looked it up: there are over 19,000 FDA approved prescription drugs. We tend to take more medicine the older we get. Sometimes in the calm stretches of shared call, doctors might joke aloud the best drugs for a post-apocalyptic world. I will bring the Ativan.
The best selling drugs of all time treat the most common American maladies — too much cholesterol, too much blood pressure, too much blood sugar.
The highest grossing drugs of all time fetch a pretty penny and have multiple approvals. Abilify, an antipsychotic that was also FDA approved as an add-on for treating depression, was a top grossing psychotropic. It is generic now, however copycats continue to spawn. Humira, a monoclonal antibody useful for treating rheumatic diseases, was recently a top grossing pharmaceutical. Generally, drug patents allow a pharmaceutical to remain BRAND NAME for about 20 years. There are plenty of tricks-of-the-trade to stretch beyond 20 years.
Sometimes drugs flop, like bad movies, while others become cult classics. Pharmaceutical companies are not opposed to creativity, like Pfizer with Neurontin (gabapentin). Neurontin has a short FDA approval list, but sees prolific use due to some controversial and unscientific claims. Pfizer has paid hundreds of millions of dollars in settlements due to violations of anti-trust laws and off-label promotion. Gabapentin continues to see use for almost everything except its FDA approvals. Pfizer really went for it with Neurontin! Two thumbs down from the critics, but audiences rave at the box office.
Package Inserts
In a previous note I briefly referenced a patient responsibility. Navigating the American Healthcare System has been a series on empowering patients via patient insight. Information remains free, but misinformation abounds. Therefore I direct the responsible patient to the package insert.
It unfolds like a desert roadmap. The unwieldy double-sided print has everything you could ever want to know about the drug. It even includes probabilities. I direct the patient eye to three pieces of information: the name of the drug, the doses of the drug, and the approved uses of the drug. This is a 5 minute demystification technique. Practice saying the name aloud — made up words have made up pronunciations — have some fun with it.
Dosage and Frequency
Prescriptions all come with instructions. These are mostly standardized in the modern electronic-prescribing world: The name of the drug, the mass or density, how much to take, how to take it, and how often to take it.
A July intern ordering acetaminophen for a patient might get some nurses to laugh by accidentally selecting one of the non-oral administration routes. It might look something like this:
Acetaminophen 325mg tabs, take 2 tabs per rectum every 6 hours.
The second year resident will chuckle with the nurses and then correct the order:
Acetaminophen 325mg tabs, take 2 tabs by mouth every 8 hours as needed for moderate pain.
The point is that doctors, pharmacists, and nurses understand a standardized method of ordering and administering medication. The prescription bottle has the instructions printed on the side, so feel free to double check as often as needed.
Adherence
I know all patients omit, lie, forget, and embellish. I have done all of those things with my doctor, too. Yet I am sure we can all agree that medicine has a much better chance of working when it is adhered to as written in the prescription. Most drugs require repeat doses to have the goal effect. The winningest drugs are the easiest to adhere to. Daily dosing of a single tablet with no apparent side effect is the best. Not all drugs are so expertly designed. There is an inverse relationship among variance-tedium-frequency and adherence.
I am making a claim based on experience: Drug adherence improves with a pill organizer. It is a $1 intervention.
I recommend getting a pill box that can be loaded for the week, then putting the box in the way of some other already existing daily habit, such as on top of the toothbrush. It can take a few weeks to a few months to form a new habit.
Drug adherence is so important because without adherence all that can be garnered is the placebo effect. The whole point of going to all the trouble of seeing a physician is to get more out of treatment than just the placebo effect.
If the drug is unpleasant, unwanted, or too difficult to take, then please tell the doctor. Some doctors make patients feel bad for not following instructions (they think this will help the patient better follow instructions (this is bad psychology)). Most of the time the doctor can make better informed treatment recommendations if a patient is forthcoming about drug adherence. I apologize in advance if honesty yields a scolding lecture, but I still think honesty is the best policy.
Cost
Medicine can be dirt cheap or outrageously unaffordable. Generic drugs trend towards inexpensive and branded drugs often go for more than a monthly car payment. The cost to the consumer depends on the pharmacy, insurance plan, and diagnosis. You have heard it takes two to tango? Prescribing a drug is a square dance with lots of partners to spin around.
The prescriber and the patient discuss the medicine together and the patient agrees to try the drug.
The prescriber sends the e-script to the pharmacist, who then checks the patient’s insurance coverage.
Often the drug is covered by insurance, and then the pharmacist charges the patient the drug co-pay per the insurance plan.
Sometimes the drug might be covered but requires approval. This is known as “prior authorization,” also referred to as “PA” or “prior auth.”
The prescriber will need to fill out the PA form and send it back to the insurance company for review.
If the insurance company approves the authorization then the drug is covered by the insurance company and the pharmacist is paid to fill the script.
If the PA is denied then the prescriber can appeal that decision, or prescribe something different, or recommend the patient absorb the cost.
Either of the latter two options means the insurance company is not paying the pharmacy for filling the script.
By the way, a drug is covered or not covered independently of who prescribed it. In other words, it does not matter whether or not the prescriber bills the insurance company for the visit — the drug coverage is related to the insurance formulary.
The documented diagnosis matters when a drug is expensive and the insurance company wants to ensure it is being prescribed for something the drug treats and no cheaper alternatives are available.
The specific pharmacy affects the price of the drug as well for a couple reasons that are tedious so I will sum it up:
Distributors negotiate with manufacturers
Pharmacies negotiate with distributors
Insurance companies have preferred pharmacies, and utilize pharmacy benefit managers to set prices on insurance plans
The pharmacist is part of your healthcare team. They save patients from harm by preventing dangerous drug combos, fixing incorrect orders, and monitoring all of the medicine incoming from various prescribers. Do talk to your friendly neighborhood pharmacist and let them get to know you. Bonus: they will help you on cost saving often enough as well.
Chemistry
Biology is remarkable at maintaining homeostasis. Chemical chains and folds form proteins, proteins make up cells, cells form tissues, tissues form organs, and organs form organisms. The human body is perpetually in a state of change, but always resisting change. When a medicine is ingested, the body responds immediately to eliminate it — perhaps you took some acetaminophen for a headache and noticed the headache went away but came back the next day. All of the acetaminophen was cleared from the body and the headache returned.
The ways in which the body acts on the drug is called pharmacokinetics. The inverse, how the drug acts on the body, is called pharmacodynamics. The rate of drug clearance is often referred to as a “half-life.” The intended pharmacodynamic effect is often referred to as “the effect.” The unintended pharmacodynamic effects are often referred to as “side effects.”
Imagine a pie eating contest between two brothers. Their mothers had interesting choices for names: Zeroth and First.
“Zeroth” eats pies very consistently. Exactly 10 pies an hour, every hour, until all the pies are gone. 100 pies takes him 10 hours to eat. 1000 pies takes him 100 hours to eat, etc.
“First” has a different strategy. “First” will survey the total number of pies and make two even piles, then he will eat all of one pile in one hour. If there 100 pies then “First” eats 50 pies in an hour. Now he has a remainder of 50 pies, which he splits evenly and consumes 25 in an hour. He repeats this until all of the pies are gone. Be it 100 pies or 1000 pies, First will finish everything in about 6 hours.
When it comes to pie eating, Zeroth makes more intuitive sense, but zeroth order kinetics are uncommon in the body. First order kinetics rule the day. The main exception to know is alcohol (ethanol), which is cleared by zeroth order kinetics, meaning a consistent rate per hour regardless of total volume.
First order kinetics operate on half-life clearance as previously referenced. It takes about 5.5 half-lives to clear a drug by first order kinetics. Thinking of First, our champion pie eater, he eats 50 pies the first hour, 25 pies the second, 12.5 pies the third, 6.25 pies the fourth, and 3.125 pies the fifth. By the end of five hours, out of 100 pies there are only 3.125 pies left.
Zeno was a philosopher who was unaware of calculus, but calculus proves that First will eat every last pie crumb… in the human body think of it as First giving up and Zeroth coming over to eat the leftovers after 5.5 half-lives.
This is important because it provides insight into how to take a drug and how to discontinue a drug. Enzymes in the liver are primarily responsible for “detoxification.” These enzymes respond to the drug as an unwanted toxic invader and immediately begin clearing it out! By consistently taking the drug we can overpower the detoxifying enzymes and gain the benefit. Discontinue the drug and it will take 5.5 half-lives to be fully eliminated.
A principle of medical detox is to never decrease a drug that is harmful in withdrawal by more than 50% per half-life. See the package insert for more info on the specific half-life.
Pharmacodynamics teaches us dose response curves. They often look sigmoidal like this:
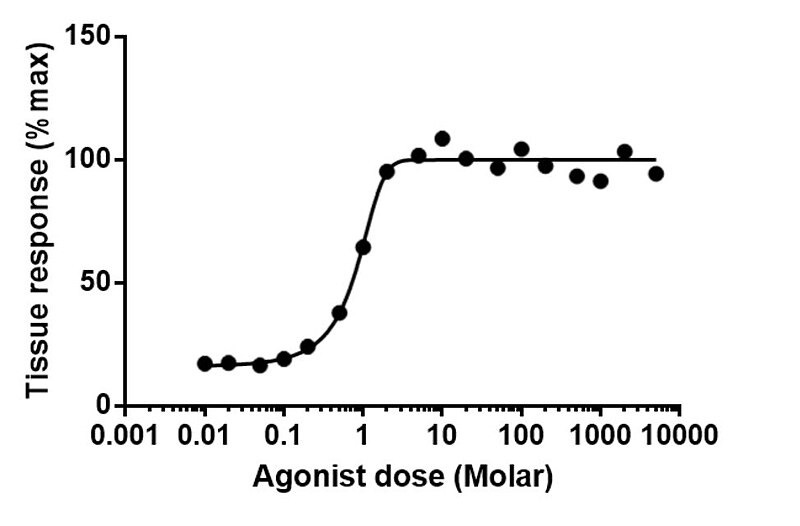
As the dose of a drug increases logarithmically we start to get a target response. As you can see on the curve, multiplying the dose by 10 does not result in 10x the response, and eventually the response plateaus even with a 1,000 times dose increase. There are upside down U shaped curves, double sigmoids, and linear curves, but most dose response curves are like the one above.
Another pharmacodynamic principle to be aware of is LD50. This refers to the dose of a chemical that is lethal to 50% of organisms exposed (tested on various lab animals). Achieving a target response while staying many orders of magnitude below LD50 is a common sense requirement for any therapeutic pharmaceutical. This is where the saying “the dose makes the poison” is the most useful. Water has an LD50 of 90g/kg in rats. Every chemical has some hypothetical LD50 as the LD50 is a physical property of biochemistry.
Side Effects and Drug-Drug Interactions
Side effects references the phenomena of unintended response. The target effect is ideally disease modifying or symptom reducing. A “clean drug” has very little effect outside of the target receptors. A “dirty drug” interacts with many more receptors than intended.
Many drug uses were discovered through side effects. Serendipity does a lot of heavy lifting in science.
The patient (generally) gets to decide if a side effect is tolerable or intolerable. The tolerability of a side effect tends to relate to the harm and/or hurt of the underlying illness. If an illness is deadly or very painful then treatments might ethically become more prodigious.
Pleasant feeling side effects can also be hazardous, as physical and psychologic rewards are risk factors for an addiction side effect.
Generally, it is better to avoid adding medication to diminish side effects of the initial medicine, nevertheless polypharmacy is sometimes necessary in healthcare. Disease states tend to determine other disease states the same way toppling dominos crash into each other. Reversal of a disease state may require multiple interventions.
If you take two or more drugs then you might experience special side effects known as drug-drug interactions. Some drugs speed or slow metabolism of other drugs. One drug in particular, carbamazepine, induces its own metabolism. It is a snake eating its own tail.

Did the ancient alchemist scribe ever imagine a future human would use his drawing (above) to reference a compound that treats epilepsy?
I do have a question about antipsychotics though…. Haven’t studies shown that they are often obesogenic, can cause uncontrollable movement, and long term decrease white matter in the brain? Why are these drugs prescribed so much if they cause so many adverse side effects?
Nicely done! Thank you for putting this information out there.